The AMA/Specialty Society Relative Value Scale Update Committee (RUC) values physician work for new and revised CPT® codes, reviews practice expense inputs associated with codes being valued, and assists CMS in reviewing codes identified in various screens.
The ACR has representation on the RUC and submits recommendations on radiology-related codes.
Relative Value Scale Update Committee (RUC)
|
|
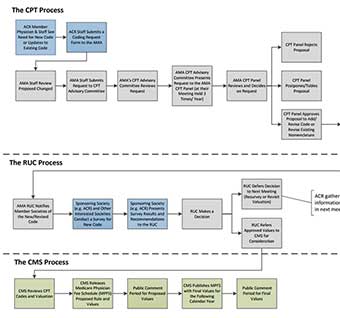
The Relative Value Scale Update Committee (RUC) is responsible for valuing physician work for new and revised CPT® codes.
With the institution in 1992 of resource-based reimbursement for physician work, this committee was formed so that organized medicine would have a multispecialty group that could assess the relative physician work of the various CPT codes. Unlike the CPT Editorial Panel, which has no designated seats for specific specialties, the RUC has seats for the major specialty organizations, including Radiology.
Gregory Nicola, MD, FACR, is the Radiology RUC representative on the panel, with Lauren Nicola, MD, FACR as his Alternate. Andrew Moriarity, MD is the ACR RUC Advisor, with Michael Booker, MD, MBA as the Alternate Advisor. Unlike the CPT Editorial Panel, which makes the final decisions on the content of CPT, the RUC is an advisory body to CMS, which makes the final decision on values for each of the codes.
Like the Editorial Panel, the RUC also has an advisory committee, with members from all organizations that have a seat in the House of Delegates, including the ACR and other radiological organizations. When the Editorial Panel approves a new or revised code, all specialty societies can recommend a value for the code or comment on recommendations by others. The recommendations are developed using a formal survey process that compares the new or revised code to existing code values. Members of the ACR may be requested to participate in these surveys. If so, it is critical that the surveys be completed since the credibility of the recommended value is highly dependent on the quality of the survey.
The Medicare Physician Fee Schedule relative value unit (RVU) for any given code is divided into three components: physician work, practice expense, and malpractice cost. Congress has mandated that the practice expense component be converted from the old change-based values to resource-based values similar to the changes made for the physician work component. The implementation of this change began January 1, 1999. The RUC evaluates and recommends values for this component of the fee schedule as well and has created a standing subcommittee to deal specifically with this component: the Practice Expense Subcommittee.
Practice Expense Subcommittee
The Practice Expense Subcommittee is responsible for the refinement of direct practice expense inputs for new and revised CPT® codes.
Practice expense for all new and revised CPT codes is reviewed and evaluated through the American Medical Association's Practice Expense Subcommittee. Reimbursement for medical procedures, as defined by CPT codes, is divided into three components – physician work, practice expense and malpractice expense.
The physician work component became resource-based (reimburse for the actual cost associated with providing a service) under a "Relative Value System (RVS)" in 1992. Congress also mandated that the practice expense component become resource-based, with a four-year gradual transition, beginning in 1999. With this transition, CMS designed a two-pronged process for data collection.
The first effort by CMS was a very complex survey that failed due to inadequate response from the survey participants. The second effort by CMS was to use the Clinical Practice Expert Panels (CPEPs). These panels included representatives from all major medical specialties who identified "direct inputs" (non-physician clinical labor, medical supplies, procedure specific equipment, and overhead equipment) incurred in performing medical procedures represented by CPT codes. Congress mandated that this direct cost data be validated. In response to this mandate, CMS reassembled the CPEPs to review and evaluate data they previously developed. To this need, the AMA Relative Value Scale Update Committee (RUC) developed a subcommittee called the Practice Expense Advisory Committee (PEAC), which was primarily responsible for the analysis and refinement of the original CPEP data. Through its last meeting in March 2004, the PEAC provided recommendations for over 7,600 codes. The PEAC was replaced by the Practice Expense Review Committee (PERC) and now those PE-related activities are addressed by the AMA RUC PE Subcommittee.
The PE Subcommittee meets three times a year to review direct practice expense inputs as presented by the specialty societies and may make modifications. The recommendations presented to the PE Subcommittee represent the "typical" case scenario for practice expense for the new and revised codes, encompassing three areas: 1) Clinical staff time; 2) Medical supplies; and 3) Equipment. While some elements may seem minor, each of the three sections listed above are essential in building up a complete picture of what it costs to perform radiology services. The recommendations are reviewed and finalized by the ACR's Practice Expense Committee before they are submitted to the PE Subcommittee. Following approval by the Subcommittee and the RUC, the PE recommendations are forwarded to CMS to be used to calculate the practice expense relative values.
The ACR Practice Expense Committee was formed in 2000 in response to a mandate by the AMA PEAC that specialty societies formalize a specialty panel which reviews all data and makes final recommendations regarding the "direct inputs" of practice expense for both the office and out-of-office clinical settings. The ACR Practice Expense Committee was merged with the Economics Committee on Reimbursement in 2017.